Anyone interested in building muscle knows that adequate (or perhaps more than adequate) dietary protein (plus exercise, of course) is crucial. And marketers certainly do — just run your eyes down the shelves of protein supplements in any health food store.
This is of more than academic interest for some groups — aging men for example who are known to lose muscle mass and functional abilities as they grow older. Would it help such men maintain their lean body mass (LBM) and abilities to increase their protein intake?
Using a group of 92 older men (mean age 73 years), a group of researchers from Brighams and Women’s Hospital in and the Boston Medical Center, investigated whether protein intake above the current RDA (0.8 gm/kgm body weight) with or without testosterone supplementation would help maintain LBM and functional abilities. Testosterone is known to increase muscle mass and strength — would additional protein improve the effect of testosterone? All the men had some degree of functional limitations at the start of the study, and all had average daily protein intakes less than or equal to the RDA.
The participants were randomly assigned to one of four groups:
- 0.8 gm protein/kgm + testosterone injections
- 1.3 gm protein/kgm + testosterone injections
- 0.8 gm protein/kgm no testosterone
- 1.3 gm protein/kgm no testosterone
Packaged meals with individualized protein and calorie contents were provided to the participants — these contained 0.7 gm/kgm protein and protein supplements of 0.5 gm/kgm for groups 2 and 4. the meals also provided about 80 percent of each person’s energy requirements — the rest came from discretionary foods. The experimental protocol lasted for 6 months, and every week participants met with a nutritionist who reviewed their records of food intake.
After 3 and 6 months on their treatment plans, the men were tested on muscle performance measures as well as physical function measures, and their lean body mass was determined by the use of DEXA (dual energy x-ray absorptiometry).
Over the 6 month period, protein levels had no effect on LBM, in those who did or did not also receive testosterone injections. Testosterone, as expected, significantly increased the LBM compared to men getting placebo injections. Similarly, the amount of fat was diminished in those injected with testosterone, however the increased protein levels also significantly decreased fat mass. Further, the total body mass wasn’t changed by increased protein levels.
When functional abilities were evaluated, testosterone injections led to an increase in strength of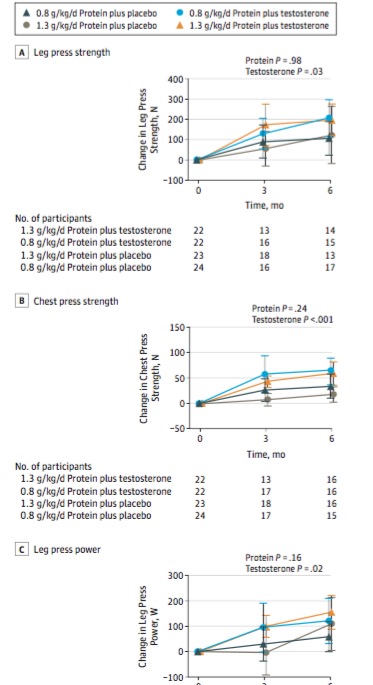 leg press and chest press power and strength, but increased protein did not, as shown in the figures.
leg press and chest press power and strength, but increased protein did not, as shown in the figures.
Thus, there was essentially no benefit to providing more than the RDA level of protein to these older men with respect to improving their functional abilities. It isn’t clear that these results would apply to other populations — younger individuals, women, or older men without prior limitations. This study does provide additional evidence that testosterone can be useful in the population studies, but that protein supplementation does not augment that improvement.
The protocol followed in this study alleviated a major problem with nutritional studies — basing results on self-reported food intakes derived from food frequency questionnaires or only dietary recalls. In this case, the participants were provided with foods carefully designed to meet their protein and energy requirements, and their adherence to protocol was closely monitored.
In sum, the investigators concluded
Protein intake equal to the RDA was sufficient to maintain LBM, muscle strength, and physical function in functionally limited older men. Our findings do not support the recommendation that protein intakes higher than the RDA promote LBM accretion or augment anabolic response to a muscle anabolic drug, such as testosterone.



