
Vaccination of high-risk groups against SARS-CoV-2, the virus that causes COVID-19, has begun in earnest – and not a moment too soon because the trends in the United States are moving in the wrong direction. On December 13, records were set for 7-day averages of daily cases ((211,494), the number of people hospitalized (106,656), and daily deaths (2,427); and with the Christmas and New Year’s holidays approaching, we can expect worsening numbers through January.
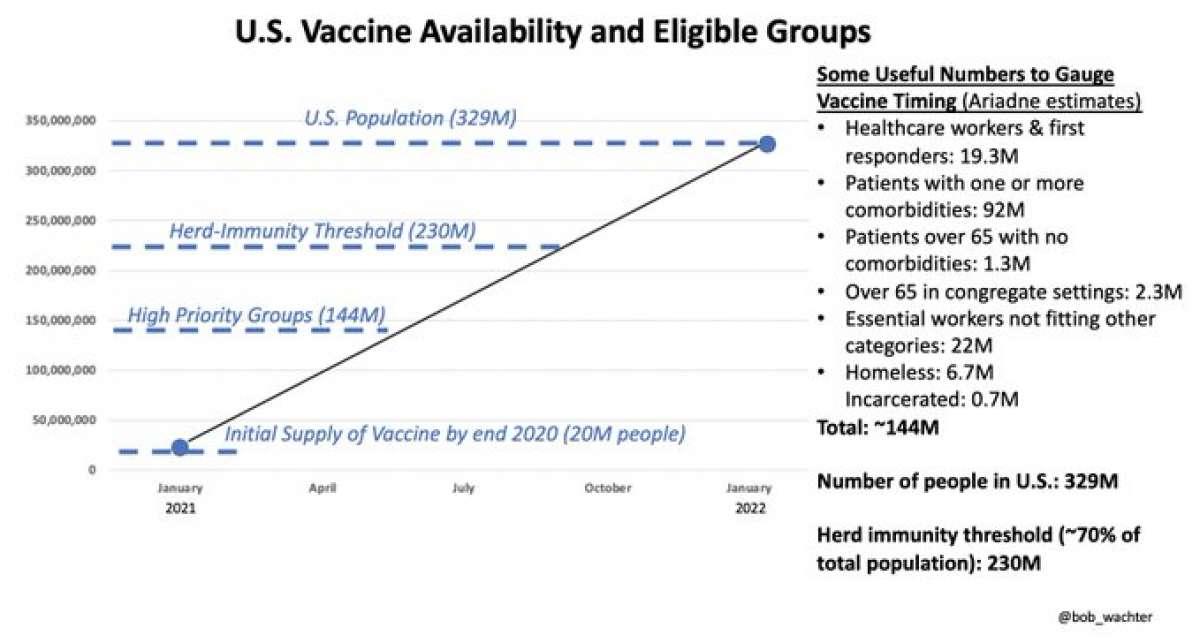
If enough people opt to take the COVID-19 vaccines – a big if – they will be a game-changer, but even in a best-case scenario, they won’t make a big dent in the pandemic for some time. According to a timeline provided by Dr. Bob Wachter, chair of medicine at the University of California, San Francisco, it might not be until sometime in the third quarter of 2021 that we reach “herd immunity,” the state when a sufficient percentage of the population has immunity from natural infections or vaccination that the virus has difficulty finding new, susceptible hosts, and the pandemic diminishes:
What should we do in the interim, given the widespread “pandemic fatigue” -- people tiring of sheltering, distancing, and the closing of businesses? We need to recall the observation of The Great One. No, not Dr. Tony Fauci of the National Institutes of Health—the other one, hockey legend Wayne Gretzky, who once explained, “I skate to where the puck is going to be, not where it has been.”
Anticipating what’s coming is critical in confronting an infectious disease, especially one whose dynamics are what many infectious disease experts consider their worst nightmare. COVID-19 is highly infectious, has a lengthy incubation period (during which asymptomatic infected persons can unwittingly shed virus and infect other people), and causes serious, sometimes fatal illness.
Those unusual characteristics of the SARS-CoV-2 virus, which causes COVID-19, and the idiosyncrasies and spectrum of presentations of the illness—from pulmonary symptoms (including pneumonia and pulmonary fibrosis) to a range of non-respiratory manifestations, (including loss of sense of smell or taste, confusion and cognitive impairments, fainting, sudden muscle weakness or paralysis, seizures, ischemic strokes, kidney damage, and, rarely, a severe pediatric inflammatory syndrome) mean that we are on a steep learning curve.
The problem is, if we react too slowly to changing circumstances, we can fall off a metaphorical cliff. There’s an old brain teaser that perfectly illustrates this point. Consider a pond of a certain size, on which there is a single lily pad. This particular species of lily pad reproduces and duplicates itself once a day so that on day 2, you have two lily pads. On day 3, you have four; on day 4, you have eight; and so on. Here’s the teaser: if it takes the lily pads 48 days to cover the pond completely, how long will it take for the pond to be covered halfway?
The answer? 47 days. In just 24 hours, between day 47 and day 48, the lily pads would double in size and overtake the pond. Moreover, on day 40, the pond would still appear to be relatively clear; just eight days from the pond being completely covered, you’d hardly know the lily pads were there.
If the same thing happens with a virulent and highly contagious infectious agent like the SARS-CoV-2 virus, you don’t know you’re in trouble until you wake up one morning to find that you’re overwhelmed. Similar to the lily pad example, the 7-day moving average of cases of confirmed COVID-19 cases in the U.S. was around 77,000 on October 29, and just six weeks later, on December 14th, it had shot up to over 214,000. During the same time period, the 7-day average of COVID-19 deaths rose from around 800 to over 2,400.
If we are to avoid even a worse impending catastrophe, we need to return to the public health mantra that was repeated endlessly in the spring: “flatten the curve.” That important concept, which was in vogue several months ago, seems largely forgotten today.
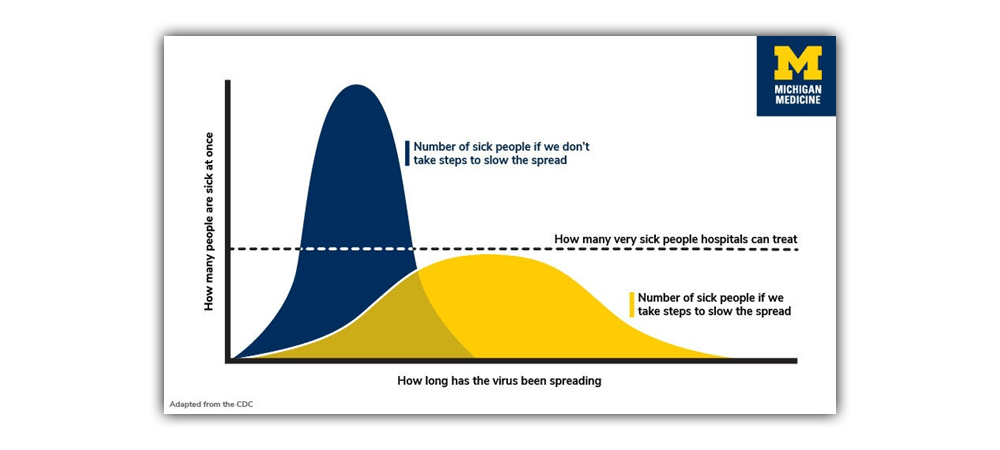
Source: University of Michigan
In the above graphic, the blue curve is the viral equivalent of the lily pads, suddenly covering the pond. It represents a large number of people (shown on the vertical axis) becoming infected over a short time (horizontal axis), and, in turn, overwhelming our health care system with people who need hospitalization, or even an Intensive Care Unit (ICU).
If, however, political officials, individuals, and communities take steps to slow the virus’s spread, the cases of COVID-19 will stretch out across a more extended period, as depicted by the flatter, yellow curve. As long as the number of cases at any given time doesn’t bleed past the dotted line marking the capacity of our nation’s health care system, we’ll be able to accommodate everyone who is very sick. Currently, many people who need treatment in an ICU are being accommodated in “step down units” or in makeshift ICUs in recovery rooms attached to operating rooms.
Curve-flattening has fallen out of focus in recent months, in part because some political leaders reopened too aggressively and prematurely, basing policy on their constituents’ “pandemic fatigue,” instead of on the advice of epidemiologists and infectious disease experts. Many people have chosen to reject good public health practices, such as wearing masks, physical distancing, frequent hand-washing, and avoiding traveling, family get-togethers, and crowded indoor places.
However, it’s still critical to avoid practices that will get us to the pattern of the blue curve, not only to spare hospitals and ICUs—which are currently under stress in many parts of the country but also so that we can continue the gradual reopening of the nation’s businesses and schools. Reopening relies on curve-flattening. As the NIH’s Dr. Tony Fauci says frequently, public health and economic considerations are not in opposition but are opposite sides of the same coin; we can’t fully restart and resume commerce until the pandemic is under some measure of control. When numbers of new cases, hospitalizations, and deaths are soaring, people won’t go to shops for non-essentials, fly, patronize restaurants, theaters, and athletic events, or send their kids to school.
That means we need to start anticipating and stop playing catch-up—as many governors having been doing, relying on a combination of magical thinking, misguided prattle about “individual choice,” and too-little-too-late remedies, instead of aggressive, evidence-based public health policies. Elected officials must heed Wayne Gretzky’s admonition and stay ahead of the coronavirus, in order to lower its rate of transmission. That’s the only way to slow the rise of new cases.
Evidence-based policies, such as requiring masks in public, prohibiting large indoor gatherings, and indoor dining at restaurants, are important. But as we’ve seen with California, even aggressive imposition of those kinds of strictures has not been sufficient—in large part because many people, especially younger ones, have failed to comply. As California allowed businesses and public places to reopen, bars, boardwalks, and beaches became crowded with large numbers of maskless patrons. It’s no wonder, then, that in many parts of California, ICUs (and especially, their professional staffs) are under stress, and as a result, Governor Gavin Newsom has had to reimpose widespread restrictions on commerce and individuals’ activities.
We won’t get to the point of herd immunity and some semblance of normalcy without some hardship in the form of sensible, science-based, government-mandated restrictions -- and widespread public compliance with them. When we can finally see the faint light at the end of the tunnel, this isn’t the time to let up.
Henry I. Miller is a physician and molecular biologist. He was formerly a Research Associate at the NIH and the founding director of the Office of Biotechnology at the FDA. Find him on Twitter @henryimiller.

Henry I. Miller, MS, MD
Henry I. Miller, MS, MD, is the Glenn Swogger Distinguished Fellow at the American Council on Science and Health. His research focuses on public policy toward science, technology, and medicine, encompassing a number of areas, including pharmaceutical development, genetic engineering, models for regulatory reform, precision medicine, and the emergence of new viral diseases. Dr. Miller served for fifteen years at the US Food and Drug Administration (FDA) in a number of posts, including as the founding director of the Office of Biotechnology.



.jpg){kind=link}