
This protocol has worked well for some pollutants, for which concentrations are now well within standards:
- carbon monoxide (CO)
- sulfur dioxide (SO2)
- lead (Pb)
However, ozone (O3), nitrogen dioxide NO2), and particulate matter (PM) are different.
- Ozone is not emitted directly but is formed by chemical reactions in the atmosphere, often far downwind.
- Any combustion process can produce NO2 at sufficiently high temperatures.
- PM is defined solely by particle size and can have any chemical composition, including combustion products, pet dander, floor sweeping, or the personal “clouds” around individuals.
Each of us operates and controls our personal sources of NO2 or PM outside of the regulatory framework. Our “ambients” include where we live, work, and travel; why focus on the outdoors?
“None of the epidemiology studies used to support EPA ambient air quality standards were based on actual (personal) exposures.” [1]
This was true in 1999 when I wrote it and remains so today. EPA’s air pollution control programs are based on community-average outdoor air quality since it was felt that considering individual personal exposures could be intrusive. This might have been acceptable when control programs began, and relief from the outdoors could be found indoors. Today’s indoors, where we spend ~85% of our time, may not always be cleaner because of domestic NO2 and PM emissions.
Personal PM exposure (PMpers) has been defined as emissions from indoor sources (PMin) such as smoking, cooking, cleaning, pets, or candles, plus outdoor air that infiltrates or enters the home (PMinfil). Indoor emissions are influenced by the properties of residential structures and pollution-producing activities of occupants; controlling indoor rather than outdoor air pollution could be more beneficial.
Simulated Long-term Analysis
I examined the epidemiological implications of using personal exposures rather than outdoor PM concentrations [2] to predict changes in life expectancy at birth, expressed as years of life per unit of PM concentration – the dose-response function (DRF).
Lacking current data on infiltration rates and indoor air quality, the PMin, I postulated a mean rate of infiltration of 50% and alternative levels of PMin: one equal to the outdoor infiltration and one twice that level as might be produced by second-hand smoke. I randomized state-level values to simulate house-to-house surveying. [3]
From these simulations,
- The baseline DRF was based on measured outdoor PM2.5, with a mean of 11.8 μg/m3 and a range of 5.2-17.2 μg/m3 across the 49 states.
- This resulted in infiltrated outdoor air, PMinfil, contributing a mean of 6.6 μg/m3 with a range of 0.93-13.2 μg/m3.
- Indoor sources, PMin, contributed a mean of 5.8 μg/m3 with a range of 0.053 - 14.8 μg/m3.
- In the low-exposure scenario, personal exposure was 11.9 μg/m3. In the high-exposure, smoky scenario, that value rose to 17.5 μg/m3.
- These mean personal exposure levels were similar to outdoor PM2.5, but their ranges across the group of 10 were much larger, from 4-fold for the low-indoor-pollution case and 9-fold for the high-indoor-exposure case.
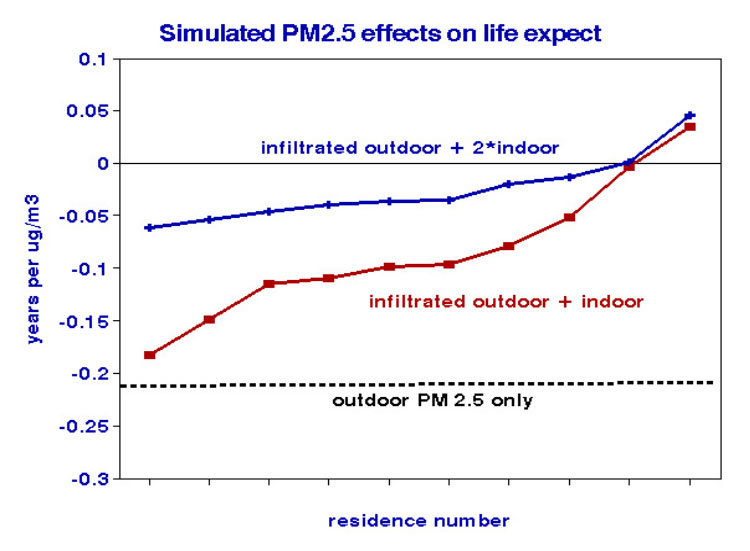 I then estimated life expectancy DRFs for ten hypothetical households with varying outdoor exposure and infiltration rates using the 49-state distributions of PM as the sole predictor. Life expectancy declined by 0.21 years for every unit increase in PM. Those life expectancy changes, measured by personal exposure, varied from a loss of 0.18 to a gain of 0.025 years per PM unit (see graph). The average change for these ten hypothetical households was 0.17 years lost, 90% less than that calculated based solely on outdoor pollutants as is done by the EPA.
I then estimated life expectancy DRFs for ten hypothetical households with varying outdoor exposure and infiltration rates using the 49-state distributions of PM as the sole predictor. Life expectancy declined by 0.21 years for every unit increase in PM. Those life expectancy changes, measured by personal exposure, varied from a loss of 0.18 to a gain of 0.025 years per PM unit (see graph). The average change for these ten hypothetical households was 0.17 years lost, 90% less than that calculated based solely on outdoor pollutants as is done by the EPA.
Timing Issues
Short-term (daily) responses to brief pollution episodes are not an issue since outdoor peaks are attenuated indoors and unlikely to coincide with peaks in indoor emissions. By contrast, exposures over decades are required to estimate chronic effects, during which outdoor air quality is likely to have improved, unlike indoor emissions. As a result, personal exposure differences are likely to worsen over time.
Implications
Dose responses are likely to be overestimated when based solely on outdoor or indoor exposures. Similarly, neglecting a significant portion of exposure will mask any dose threshold that might exist. Epidemiology’s failures to find thresholds in responses to outdoor PM2.5 while neglecting indoor PM2.5 has led to never-ending futile demands to reduce outdoor emissions. The correct procedure would be to evaluate dose responses for outdoor and indoor PM jointly, each involving different constituents of PM2.5 and relevant toxicity. It is also likely that confounding by socioeconomic variables like income or education will differ between indoor and outdoor PM.
This analysis demonstrates what is intuitively obvious: that assigning health effects to air pollution requires detailed knowledge of total exposures. We should each be responsible for our micro-environments; governments could help by providing information on common indoor air pollution hazards.
[1] Statistical Considerations in Determining the Health Significance of Constituents of Airborne Particulate Matter Journal of Air and Waste Management DOI: 10.1080/10473289.1999.10463896
[2] The data set included state-level data for the contiguous United States and the District of Columbia.
[3] Random numbers produced alternative statistical exposure distributions, resulting in a mean of 0.55, a maximum of 0.99, and a minimum of 0.014. This process was repeated ten times to simulate distributions


