The U.S. Office of Inspector General (OIG) has estimated that in calendar year 2013, $359 million (82%) of $438 million paid to chiropractors under Medicare Part B did not comply with Medicare requirements.(1)
Since 1973, Medicare has covered manual manipulation of the spine for the treatment of certain neuromusculoskeletal conditions. Its policies are set by the Centers for Medicare & Medicaid Services (CMS), a branch of the U.S. Department of Health & Human Services. To get paid, chiropractors are supposed to (a) specify the region of the spine where the supposed problem exists, (b) diagnose a medically recognized condition that is related to that spinal region, (c) document symptoms, physical findings, and/or x-ray findings that are related to that region, and (d) record a treatment plan that specifies goals and objective measures to evaluate treatment effectiveness. The chiropractor must also attest that the patient is receiving “active” treatment, which is defined as a “reasonable expectation of recovery or improvement of function.”
Services intended to prevent disease, promote health, prolong or enhance the quality of life, or maintain or prevent deterioration of a chronic condition are considered “maintenance care” and are not covered. Chiropractors are notorious for urging patients to keep coming for “corrective” and “wellness” care after their initial symptoms have resolved. The true percentage who routinely do this remains unknown but it is not small.
Most people who might benefit from spinal manipulation are patients with acute low back pain or neck pain. Such problems seldom require more than a few sessions in which manipulation is applied to one or possibly two regions of the spine. Patients with chronic back or neck pain who might benefit from spinal manipulation might need more, but active treatment seldom requires more than 12 sessions and rarely requires more than 24.
The recently released study, which applied strict criteria to a sample of patient records, concluded that (a) among patients who were seen 1 to 12 times, only 24% of services were justifiable, (b) only 5% of visits number 13 to 30 were justified, and (c) no services over 30 per patient should have been paid for. The estimated unallowable payments were $228.7 million for the 1-12 group, $101.4 million for the 13-30 group, and $28.7 million for the over-30 group.
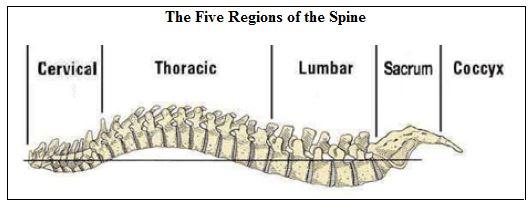
To bill for their services, chiropractors must use one of three Current Procedural Terminology (CPT) codes:
⦁ 98940 (for manipulation of 1 or 2 two regions)
⦁ 98941 (for manipulation of 3 or 4 regions)
⦁ 98942 (for manipulation of 5 regions)
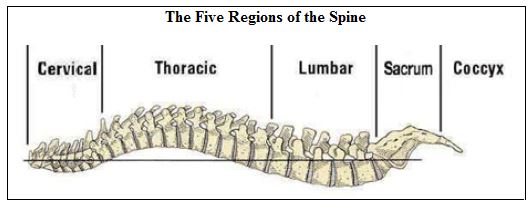
Very few conditions require treatment of more than two spinal regions. For example, people with low-back pain are unlikely to neck manipulation; and people with neck pain are unlikely to need low-back manipulation. Thus, most claims for 3- or 4-region manipulation are questionable and all claims for 5-region manipulation should be highly suspect.
To increase Medicare payments, many chiropractors manipulate more regions or than necessary, treat more frequently than needed, and/or report treating more regions than actually treated. Some also try to conceal the fact that they are providing maintenance therapy by changing their diagnosis every 12 visits.
Since 1986, the OIG has issued at least 15 reports about improper payments to chiropractors. Taken together, the reports indicate that despite 30 years of obvious problems, CMS administrators have done a very poor job of screening out improper claims. The October 2016 report recommends that Medicare determine reasonable numbers of services that are necessary to actively treat problems and implement a system that can identify and review claims in excess of those numbers. To me, this sounds both logical and simple. However, although the CMS plans to look more closely at the claims of high-utilizers, it says that broad limits can’t be implemented because no medical evidence exists on which to base such limits.
CPT data for 2014 can be viewed at https://projects.propublica.org/treatment/uniqservices/ by inserting each code after the forward slash. From there is it possible to identify the top billers of that code in each state and pick out hundreds who are overbilling. Data for 2012 and 2013 are available on the CMS Web site, but the interface is not user-friendly and requires expert knowledge to harvest the data for statistical study.
It would be simple to ban payments for CPT code 98942 and to implement pre-payment screening of claims from chiropractors who bill all or nearly all of their visits with 98941 or 98942. However, no such measures appear to be under consideration.
References
(1) Hundreds of millions in Medicare payments for chiropractic services did not comply with Medicare requirements. OIG report A-09-14-0233. October 2016
This article first appeared in Priorities magazine, which is sent free of charge to all American Council on Science and Health donors.



