
Here are five things we really don't need:
- Further restrictions on prescription opioid drugs. They have been a disaster by any measure. (1)
- More power for the DEA to misuse.
- Forcing doctors and other healthcare providers to effectively become another arm of law enforcement.
- Further erosion of our rights to a personal and private relationship with our doctors.
- A bunch of chuckleheads who passed a law making all of this possible.
Unfortunately, as of October 23rd, we got all five. There is some scary stuff going on. One of the physicians who I collaborate with gave me an early heads up about an atrocity that just became reality thanks to a misguided and misnamed law. The atrocity is called Suspicious Orders Report System (SORS), and if this conjures up memories of Stalinist Russia, where everyone was spying on everyone else, you're not alone.
Original image: Asia News
SORS came into being thanks to a new law called Substance Use-Disorder Prevention That Promotes Opioid Recovery and Treatment For Patients And Communities Act, aka, Public Law 115-271 115th Congress. The law was introduced in 2018 by Representative Greg Walden (R-OR). It can't be the least bit surprising that this dangerous law originated in Oregon (2).
In case you haven't noticed, the acronym for the Substance Use-Disorder Prevention That Promotes Opioid Recovery and Treatment For Patients And Communities Act is the SUPPORT Act. I really hate to use Stalin and Orwell in the same article (so trite) but it is unavoidable here.
SUPPORT????? Are they kidding? It is anything but, something that will quickly become obvious in a moment.
Earlier this week I wrote about a report in Public Health Reports, the official journal of the Office of the Surgeon General), (2) which concluded in no uncertain terms that prescription opioids play only a very minor role in overdose deaths in the US – something that has been obvious for quite some time.
So, perhaps this country will finally come to its senses, right?
No. Quite the opposite.
Here's what Greg Walden and his comrades buddies came up with. It's horrifying.
- Distributor
- Manufacturer
- Importer
- Pharmacy
- Hospital/Clinic
- Teaching Institution
- Practitioner
- Mid-Level Practitioner
- Mid-Level Practitioner-Ambulance Service
- Researcher
- Analytical Lab
- Narcotic Treatment Program (NTP)
In other words, anyone who might get within one zip code of a Vicodin pill will be required to report any of the following "suspicious acts" to the SORS Gestapo, where it will go into a database.
"The SUPPORT Act states the term “suspicious order” may include, but is not limited to":
- An order of a controlled substance of unusual size
- An order of a controlled substance deviating substantially from a normal pattern
- Orders of controlled substances of unusual frequency
When the physician, who wisely wishes to remain anonymous, wrote to me he/she also included some comments along with his/her email (emphasis mine).
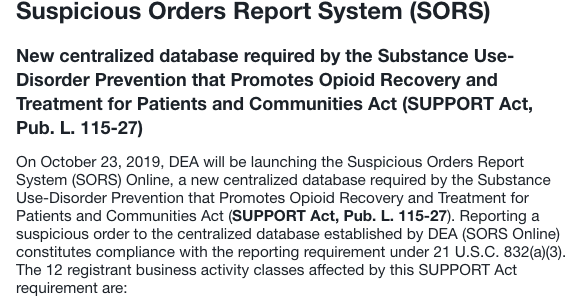
The DEA has launched a new program as part of the initiative to discourage legitimate prescription of opioid analgesics.
The Suspicious Orders Report System (SORS) is a new online centralized database required by the Substance Use-Disorder Prevention that Promotes Opioid Recovery and Treatment for Patients and Communities Act. Pharmacies, hospitals, clinics, doctors and even EMS workers are now required to report a “suspicious order” to the centralized database established by DEA (SORS Online).
A “suspicious order” may include, but is not limited to: an order of a controlled substance of unusual size; an order of a controlled substance deviating substantially from a normal pattern, and; orders of controlled substances of unusual frequency constitutes compliance with the reporting requirement under 21 U.S.C. 832(a)(3).
Doctors beware, Big Brother DEA is watching you.
Anonymous, October 23, 2019
My take? The DEA has failed miserably in keeping illicit fentanyl and its analogs out of this country (3) so the agency, like lawmakers, has doubled down on pills, even as more and more evidence emerges that pills are not only not the primary (or even close) culprit in causing overdose deaths, but there is a real inverse relationship between the number of prescriptions and overdoses, something I have written about numerous times in the past.
So, pain patients, already suffering mightily because they can no longer get the medications they need, will suffer more. Doctors, who are already being targeted by law enforcement agencies for trying to do their jobs properly will face additional pressure to not prescribe painkilling medications. And addicts, who have been dying in increasing numbers as pills become harder to come by, will be sitting ducks for street fentanyl. OD deaths will continue to rise and probably even more so because the people who really need help and support will instead get SUPPORT.
There isn't much more to say.
NOTES:
(1) See Gee, Pain Pills Are Not Killers. And The Sun Rises In The East. Who Knew?
(2) Oregon is arguably the cruelest state in the nation for pain patients. See Shades Of Tuskegee - Oregon's Monstrous Experiments On Poor Pain Patients
(3) To be fair, keeping illicit fentanyl out of the US is just about impossible. It is easy to make and transport, hard to detect, and you don't need a lot of it because of its potency. I have to cut DEA a break here. But to project success by going after pills, something that is rather easy to do is wrong on every level. If X punches you in the face you don't hit Y.

Josh Bloom
Director of Chemical and Pharmaceutical Science
Dr. Josh Bloom, the Director of Chemical and Pharmaceutical Science, comes from the world of drug discovery, where he did research for more than 20 years. He holds a Ph.D. in chemistry.


