
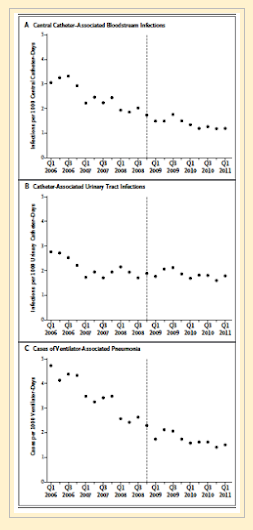
Back in 2015, the Harvard group published an extensive study on the effects of Medicare’s punitive non-payment system for hospital-acquired infections. The authors surveyed almost 400 hospitals or hospital systems for up to a total of over 28,000 unit-months. They surveyed catheter-associated urinary tract infections and catheter-related bloodstream infections – for which Medicare had established punitive non-payment policies, and hospital-acquired pneumonia for which there were no punitive policies at the time. The results, shown in their figure reproduced below, show clearly that for all three infection types, the infection rates were already decreasing before Medicare implemented their policy and that the rate of decrease did not change after policy implementation for any infection type. I concluded from these data that hospitals had realized that hospital-acquired infections were not good for patients and not good for their bottom line before Medicare’s policies and that the punitive measures did not accelerate the hospitals’ efforts to eliminate these infections. I was especially interested in these data since the small hospital where I volunteered on their infection prevention committee had incurred a punitive non-payment the year prior to the publication of the article.
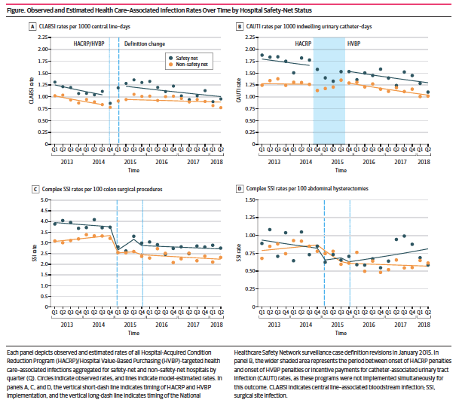
 Fast forward to 2020. Authors again from the Harvard system once again examined the effect of Medicare’s punitive non-payment policies on infection rates. They specifically compared “safety-net” and non-safety-net hospitals. “In October 2014, these programs began comparing hospital performance on selected infection metrics with national benchmarks based on prospective infection surveillance data reported to the National Healthcare Safety Network (NHSN) of the Centers for Disease Control and Prevention. At present, HVBP rewards or penalizes the highest- and lowest-performing hospitals by up to 2%of the total inpatient payments the hospital received, whereas the HACRP reduces payments by up to 1% for the lowest performers.” In this case, the team examined data from 600 hospitals who submitted their data to CDC’s National Healthcare Safety Network (NHSN) system over the years 2013-2018. Once again, these punitive measures failed to improve the rates of all four nosocomial infection types studied. The authors suggest that these punitive measures have a relatively greater financial effect on safety-net hospitals for no appreciable gain in infection prevention. They also show that Medicare has learned little over the last decade of experience since implementing these sorts of punitive measures.
Fast forward to 2020. Authors again from the Harvard system once again examined the effect of Medicare’s punitive non-payment policies on infection rates. They specifically compared “safety-net” and non-safety-net hospitals. “In October 2014, these programs began comparing hospital performance on selected infection metrics with national benchmarks based on prospective infection surveillance data reported to the National Healthcare Safety Network (NHSN) of the Centers for Disease Control and Prevention. At present, HVBP rewards or penalizes the highest- and lowest-performing hospitals by up to 2%of the total inpatient payments the hospital received, whereas the HACRP reduces payments by up to 1% for the lowest performers.” In this case, the team examined data from 600 hospitals who submitted their data to CDC’s National Healthcare Safety Network (NHSN) system over the years 2013-2018. Once again, these punitive measures failed to improve the rates of all four nosocomial infection types studied. The authors suggest that these punitive measures have a relatively greater financial effect on safety-net hospitals for no appreciable gain in infection prevention. They also show that Medicare has learned little over the last decade of experience since implementing these sorts of punitive measures.
I continue to believe that most hospital administrations understand that what is best for their patients is what is best for their hospitals and that they try and act accordingly. While I am sure that there are exceptions to this, it is clear that the Medicare policies are now doing more harm than good. In order to further lower infection rates, we probably need a better understanding of the various factors that lead to increased rates, including patient risk factors, hospital staffing, and others such that we can direct hospitals to take the measures that are required to reduce rates further.
 It is one thing to apply a general policy without regard to the specific factors one seeks to alter and another to apply specific policies tailored to the needs of individual institutions. I suggest that it is the former approach that is most needed.
It is one thing to apply a general policy without regard to the specific factors one seeks to alter and another to apply specific policies tailored to the needs of individual institutions. I suggest that it is the former approach that is most needed.



