
"People define the term differently and inconsistently. Patients don't have 'social determinants' per se; they have specific health-related social needs that impact their health and day-to-day lives. For some patients, the need might be transportation. For others, it might be housing or food insecurity."
These social determinants, like pornography, seem to be known but not so easily defined. Commonly accepted determinants include nutrition, housing, transportation, income, and access to healthcare. A few moments thought permits the realization that these determinants are entangled with one another. While more than 85% of an "Insights Council" sponsored by the New England Journal of Medicine [1] feels social determinants are important, what they are, what they do, how they will be provided, and who foots the bill is unclear.
"While data on the impact of SDOH initiatives is currently in short supply, health care leaders and clinicians are committed to its use." Dr. Namita Mohta [2]
That statement alone should give us pause. While our gut tells us that these factors are essential, you might expect some proven benefit before committing funds and further upending our concept of healthcare. But these thought leaders believe that the possible improvement in patient outcomes and satisfaction is worth the effort. They are not as convinced that SDOH will reduce or control costs, and rightly so. Here is their assessment of resources
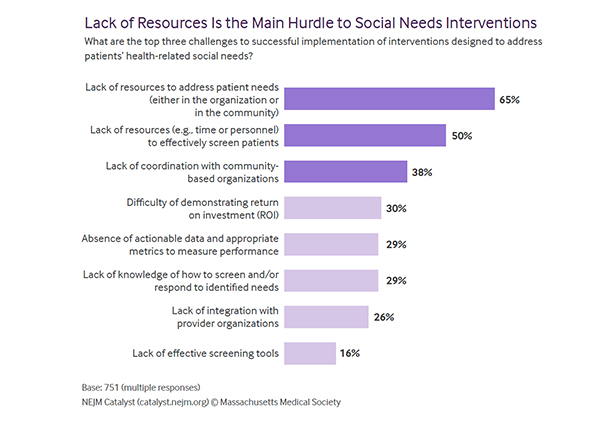 There are no resources to screen and evaluate patient needs, as well as a lack of resources and coordination with community organizations to meet those needs once identified.
There are no resources to screen and evaluate patient needs, as well as a lack of resources and coordination with community organizations to meet those needs once identified.
Given these recognized difficulties, it is an act of unfortunately characteristic hubris to hear
"The Insights Council respondents are bullish on the ability of health care organizations to scale up SDOH programs, with 71% saying it will happen over the next three to five years."
I would quickly add that this view is mainly supported by the executives who will manage these new initiatives and not the clinicians who will be tasked with doing the assessments, care coordination, and necessary follow-up. The clinicians are clear that they may well do evaluations, but the actual work of changing a patient's social determinants is not their job.
"Clinicians would love to know that there is a team member who is focused more broadly on health-related social needs, who is doing the assessment, and connecting that patient to resources. This sort of thing is not within the skill set or scope of practice of most providers, especially given all the other matters requiring their expertise and attention." Howard Eisenson, MD [3]
There is another elephant in the room of SDOH, who is picking up the tab?
 The council was pretty clear that the money was not aligned with the mouth, at least not yet. And once again, healthcare executives were twice as likely to believe the current level of funding was ample, compared to those front-line clinicians. Should more money be needed, one need only consider the words allegedly uttered by Senator Russell Long, "Don't tax you, don't tax me, tax the man behind the tree" come to mind. As you have come to expect, most members of the council felt that the individual behind the tree is you in your role as taxpayer supporting "government agencies and public payers."
The council was pretty clear that the money was not aligned with the mouth, at least not yet. And once again, healthcare executives were twice as likely to believe the current level of funding was ample, compared to those front-line clinicians. Should more money be needed, one need only consider the words allegedly uttered by Senator Russell Long, "Don't tax you, don't tax me, tax the man behind the tree" come to mind. As you have come to expect, most members of the council felt that the individual behind the tree is you in your role as taxpayer supporting "government agencies and public payers."
Social determinants of health are important, and they do make a difference. It is challenging to quarantine four people in a one-bedroom home, tough to make good food choices when McDonald's costs less than broccoli, tough to get to the doctor when you need two jobs simply to subsist, tough to navigate rapid transit when your education didn't prepare you to read a bus schedule.
But is it the role of the healthcare system to meet those needs? Dr. Eisenson is correct; physicians and nurses are not trained in this line of work. With the stay-at-home orders, it became abundantly clear that our school system functioned not only to educate but to feed and provide supervision while parents were otherwise engaged. Is that what we want for our health system? Or should we demand that the structure we have already put in place find ways to communicate better and collaborate? Just asking.
[1] The Council is an advisory group of healthcare executives, medical leaders, and clinicians asked for their opinions on various healthcare topics.
[2] Executive Editor at NEJM Catalyst, internal medicine physician at Brigham and Women's Hospital, and Assistant Professor at Harvard Medical School.
[3] Chief Medical Office, Lincoln Community Medical Center, a 10 location facility in Durham, North Caroline serving its "underserved" population
Source: Health Care Organizations Can and Must Incorporate Social Determinants NEJM Catalyst DOI: 10.1056/CAT.20.0130 and Can Social Determinants of Health Programs Be Scaled? NEJM Catalyst DOI: 10.1056/CAT.20.0129

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.


