
Flight operations for the F-35 fighter jet were suspended until further notice due to multiple episodes of apparent oxygen deprivation of pilots. Fortunately, back-up oxygen systems of the F-35A Lightning II fighters were employed successfully in all instances and the pilots navigated their planes to safety.
The U.S. Air Force takes this very seriously, as it must given the catastrophic potential of pilot hypoxia— which I will shortly describe in detail. A multidisciplinary team of experts including, but not limited to the following will be reviewing air craft technology to pilot clinical status to gear deficiencies, for instance: aerospace engineers, physiologists, aeromedical specialists, maintainers, Lockheed Martin, Naval Air Systems Command, Air Force Life Cycle Management Center, joint government and industry personnel.
Why? Because aviation physiology is complex. Tack onto that g-forces, rapid acceleration, high altitude, pressurization (or lack thereof) and the human body’s capacity under such extreme stressors. Though a remarkable machine able to adapt to a wide array of challenges, the physical and mental impact on fighter pilots requires accompanying gear and machinery necessary to support and maintain optimal health in such environs.
Gravitational Forces...
I briefly touched upon the effect of rapid acceleration (aka G-forces) in Five Great Medical Lessons from Funny Movies. You can review the video where Clint Eastwood and Tommy Lee Jone’s compete in the centrifuge test to see who passes out first. In real life, painstaking attention to detail and steps are taken to prepare a pilot for interaction with these elements. Artificial gravity testing (aka high-G training) is paramount in their training to simulate what one might experience inflight or in space. Knowing what a person’s tolerance is to these gravitational forces and building it up is a matter of life and death.
At a certain point which can vary between individuals, G-force induced loss of consciousness (G-LOC) can lead to crashes. With hypergravity states, the blood to the brain can retreat and flow outward while pooling toward the lower extremities. Angles of forces and types of training modules have different effects. There are methods to enhance tolerance and special compression suits are designed to redirect blood flow toward the upper body and head—since the brain does not fare well without oxygen if even momentarily. Additionally, fighter pilots often employ an Anti-G Straining Maneuver (AGSM) otherwise called the “Hick maneuver” to diminish the risk of blacking out. Pre-breathing treatments are vital to safety as well and must be temporally coordinated depending on the mission.
Altitude...
Then, there are the issues of altitude that we all face should we climb a high mountain or reside and visit far above sea level. The profound difference for fighter pilots is the abrupt nature of their ascent. Whereas, you may go weeks in advance to acclimate to your climb of Mt. Everest, a fighter pilot does not have that luxury and how often they exceed certain altitudes in short time spans has a long-term influence.
To understand how vulnerable even the most legendary of aerospace explorers can be, see At High Altitude with Buzz Aldrin which addresses the famous astronaut’s recent bout of altitude sickness that warranted medical evacuation from the South Pole. In Fly Me to the Moon, But Hold the Altitude Sickness I delve further into high altitude illnesses, prevention and management.
Hypoxia...
According to the Federal Aviation Administration (FAA), any individual flying above 12,000 feet in an unpressurized aircraft without supplemental oxygen is at risk of hypoxia. (1) When oxygen levels are too low or absent, the body’s tissues, blood and cells struggle to maintain normal function. The brain and nervous system are particularly susceptible to such shifts, being adversely impacted early on in the process. This can be quite insidious. As judgement and reason are compromised, danger ensues most notably from a lack of insight and self-awareness.
Hypoxia occurs when there is a failure in the pressurized system— sometimes slow, other times abrupt— or due to errors in usage or impaired oxygen support mechanisms. Human factors like alcohol or medication intake as well as level of exertion, fatigue and low blood sugar can exacerbate things too.
There are four types of hypoxia:
- Hypoxic: The most common related to altitude and with respect to flying. Caused by situations that reduce the oxygen pressure at the lung level, thereby limiting its flow.
- Stagnant: This is a circulatory transport issue where the impediment is in blood delivery of oxygen to the cells. The culprit tends to be G-forces (e.g. shock, heart failure).
- Hypemic: Any situation where blood won’t permit attachment of oxygen like in carbon monoxide (CO) poisoning. In this instance, contamination in the cabin of CO from a faulty system can compete with hemoglobin’s ability to acquire oxygen.
- Histotoxic: Caused by any interference with a cell’s ability to use oxygen effectively. Central nervous system depressants like alcohol can be problematic. Narcotics can further serve to suppress the respiratory drive.
Every person experiences hypoxia differently in terms of sequence of events. For one, dizziness might strike initially, for another headache. This is why fighter pilots are first trained in laboratory chambers to appreciate fully their personal signs and symptoms of hypoxia— the order and magnitude varies per person and traditionally remains steady with the passage of time. This helps them identify issues sooner in the future.
To observers, more labored breathing, hindered decision-making, delayed reaction time, loss of muscle coordination and bluish discoloration to the skin can be witnessed. As oxygen becomes deficient, the person can experience tingling of extremities, confusion, visual changes, headache, anxiety, euphoria, nausea, dizziness, be unable to follow commands and appropriately comprehend among other symptoms.
This audio of an actual hypoxic pilot communicating with the control tower demonstrates his disability: You will note the impaired pilot is able to declare an emergency but not appreciate the severity by indicating “other than that, everything is A-OK.” His speech is slow and sluggish and his emotional state seems euphoric. This would be the opposite response of an individual with normal mentation. You will also appreciate the alterations in altitude with respect to recovery.
In this video (also at top of article) of a military pilot in a hypobaric chamber for hypoxia training, you can observe the progression of his incapacitation. Initially, he is able to name the playing cards as he shows them to his colleagues. As the time passes, you will note an increase in the depth and rate of his breathing, he will state he feels tingling and he improperly identifies the ace of spades and other cards. His eyes don’t focus, appear glazed over and there is a disconnect between the orders he is given and his ability to perform the basic tasks. As the severity of his symptoms intensify, despite firm direction from his peers that he must do these things or will die, the subject cannot help himself and further decompensates.
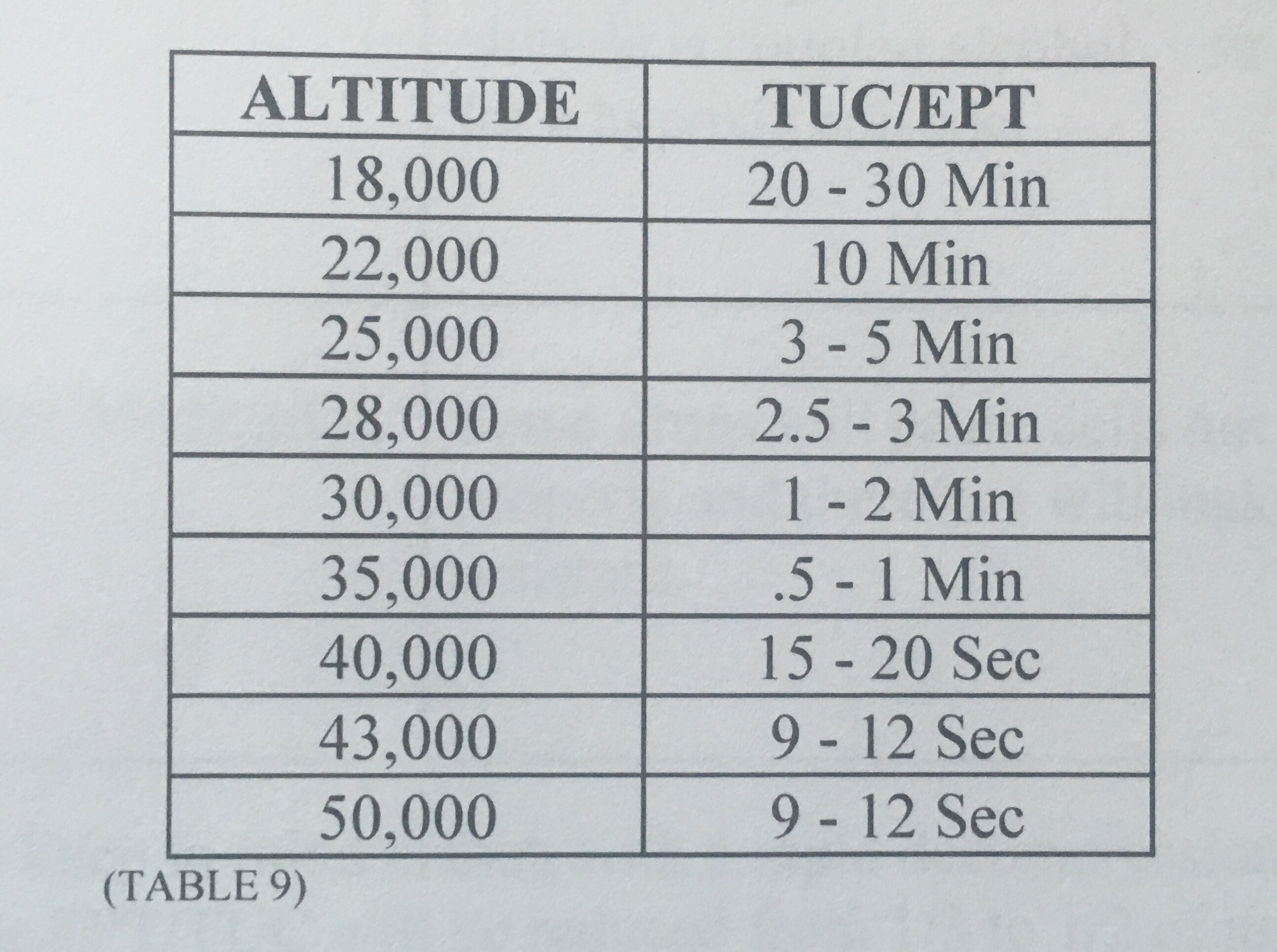
He exceeds his Time of Useful Consciousness (TUC). This is the period of time between when the oxygen is limited and he can no longer protect himself or fix the situation. The Effective Performance Time (EPT) is the period in which a pilot can perform his flying duties amidst an oxygen-poor environment.
The following table (2) shows how TUC/EPT are often used synonymously and diminish with increasing altitude. These refer to a person on average at rest. Previously described conditions that facilitate hypoxia will speed up these times.
In conclusion…
Grounding a quarter of the fleet is a sensible choice to ensure identification and resolution of the problem. The F-22 Raptor endured the same fate in 2011 until it was determined “a faulty valve on the pilots’ life support vest” was to blame as it was “improperly tightening and constricting their breathing.” Little is known so far on the source of these recent incidents other than it appears to be limited to 56th Fighter Wing pilots at Luke Air Force Base, Arizona. Hopefully, the investigation will expeditiously yield specific, correctible results.
This is also why diversity in aircraft for the military is essential. Should a technical issue arise in one design, there will be less of a burden on the remaining teams and progress can be maintained.
The success and safety of our pilots should remain the primary concern. Taking hypoxia seriously is crucial in all aspects of flight. When rapidly discovered, the threat can be resolved.
Source(s):
(1) (2) Introduction to Aviation Physiology—Federal Aviation Administration.



